Routes of Administration (ROA)
Ketamine must be absorbed into the bloodstream and circulate to the brain in order to yield a therapeutic effect. There are many ways ketamine can be administered to treat pain and mood disorders. These are called Routes of Administration (ROA) and include:
- Intravenous (IV) – direct administration into a vein.
- Intramuscular Injection (IM) – injection into the muscle.
- Subcutaneous Injection (IS) – injection under the skin.
- Intranasal – administration by inhaling a spray into the nostrils.
- Sublingual – absorption through the membranes of the mouth.
- Oral – ingestion through the digestive system as a pill or liquid
- Suppository – rectal absorption as a tablet
More on ROA
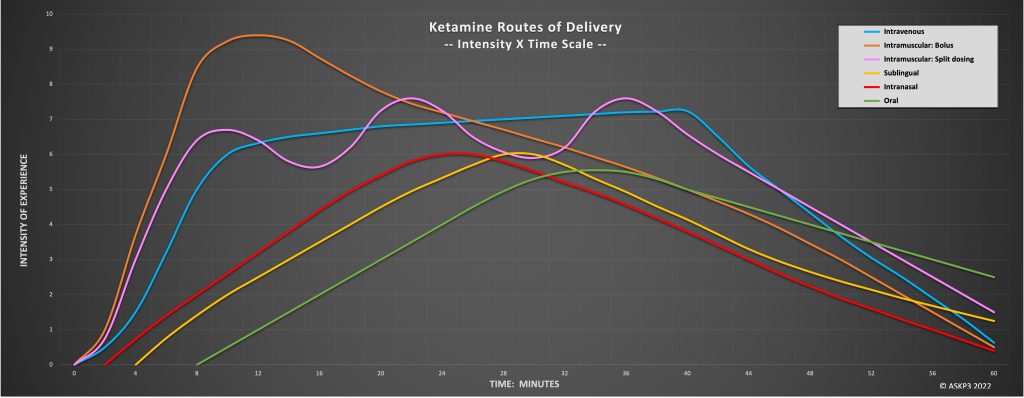
Each ROA has a different ability to be absorbed and used in the body, a term called bioavailability. As a result, each ROA has a different dosage, timing by which ketamine reaches the bloodstream, and intensity in dissociative response.
Table 1: Estimated Ketamine Formulation Dose Equivalence for different routes of administration of ketamine (Chong et al., 2009; Glue et al., 2020; Peltoniemi et al., 2016). Credit: Kelan Thomas, PharmD, MS, BCPS, BCPP
- Bio-Availability: 100%
- Peak Effect: 1 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: 35mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: 70mg
- Bio-Availability: 93%
- Peak Effect: 5 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: 38mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: 75mg
- Bio-Availability: 40-50%*
- Peak Effect: 15 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~75mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~150mg
- Bio-Availability: 40-50%* (~1.8x)^
- Peak Effect: 15 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~2 devices = 56mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~3 devices = 84mg
- Bio-Availability: 25-40%*
- Peak Effect: 20-30 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~100mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~200mg
- Bio-Availability: 25-40%*
- Peak Effect: 15-30 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~100mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~200mg
- Bio-Availability: 25-40%*
- Peak Effect: 20-45 min
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~100mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~200mg
- Bio-Availability: 15-25%*
- Peak Effect: 1-2 hours
- Dose Equivalence – .5mg/kg IV in 70 kg adult: ~200mg
- Dose Equivalence – 1mg/kg IV in 70 kg adult: ~400mg
*There may be considerable variability in bioavailability for these formulations, even across sessions
^Subjective peak effect experience may also be variable based on route and formulation since even similar plasma concentrations may have variable distribution and CNS concentration
Intravenous, intramuscular, subcutaneous, and intranasal protocols are always administered in a clinical setting. This is because the doses combined with the bioavailability often result in a strong dissociative effect, and the patient needs to be monitored in case of adverse reactions. That said, different clinics might prefer to use some ROAs over others. For example, the most studied and most often used ROA is intravenous infusion. Direct administration into the bloodstream has a 100% absorption rate and can be titrated in such a way that treatment can be slowed or stopped as needed. However, some clinics might opt to use intramuscular injections because this process is less cumbersome and expensive relative to intravenous infusions. The key difference with intramuscular injections is that there is no way to control the dose once it is in the blood stream. Further, depending on the patient’s metabolism, multiple injections might also be required to achieve the sustained dissociative state.
By contrast, sublingual, oral, and suppository administration are sometimes prescribed to be taken outside of a clinic as per the clinical judgement of the provider. Note that every State in the U.S. has different laws regarding the prescription and dosing of ketamine outside of the clinical setting. While research is still ongoing, the general purpose of these ROAs is to prolong the therapeutic effect of a clinical ketamine session (such as in the case of Ketamine Assisted Therapy) and/or to extend the period between clinic visits. These ROAs have overall much lower bioavailability and have less intense dissociative response relative to intravenous or intramuscular infusions. However, it is important that patients take care when taking ketamine in these forms as even low dosages can cause dizziness, confusion, and drowsiness. Patients taking sublingual, oral, or suppository ketamine should not drive or operate heavy machinery while under the influence of the medication.
References
Chong C, et al. Development of a SL/PO formulation of ketamine for use in neuropathic pain: Preliminary findings from a three-way randomized, crossover study. Clin Drug Investig. 2009;29(5):317-24. Glue P, Russell B, Medlicott NJ. Influence of formulation and route of administration on ketamine’s safety and tolerability: systematic review. Eur J Clin Pharmacol. 2020. doi:10.1007/s00228-020-03047-z McIntyre R S, et al. Synthesizing the Evidence for Ketamine and Esketamine in Treatment-Resistant Depression: An International Expert Opinion on the Available Evidence and Implementation. The American journal of psychiatry, 2021; 178(5), pp.383-399. doi: https://doi.org/10.1176/appi.ajp.2020.20081251 Peltoniemi MA, Hagelberg NM, Olkkola KT, Saari TI. Ketamine: A Review of Clinical Pharmacokinetics and Pharmacodynamics in Anesthesia and Pain Therapy. Clin Pharmacokinet. 2016;55(9):1059-77. doi: 10.1007/s40262-016-0383-6